Overview
The Heart Failure Society of America (HFSA) conducted a survey involving numerous heart failure providers nationwide. The survey aimed to ascertain the number of heart failure clinics in the United States and gather essential criteria about these clinics. To date, results have yielded 250 responses out of a total of approximately 500 organizations and 1,000 unique clinic locations. The survey results are summarized below.
The data presented in this article is based on information gathered in the HFSA Clinic Database Survey from July 2022 to May 2023. This data is subject to inherent limitations as the data is self-reported by the responders to the survey and has not been validated or verified for accuracy. With this said, the authors believe that the information and findings in this article are compelling and informative regarding the current status of heart failure clinics in the United States.
Clinic Information
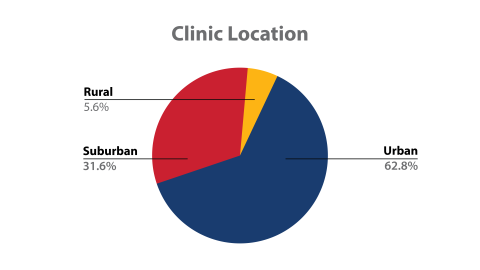
The majority of the 250 respondents' heart failure programs were in urban areas, accounting for 62.8% of the surveyed clinics. Approximately one-third of the programs (31.6%) were reported to be situated in suburban areas, while 5.6% were in rural locations.
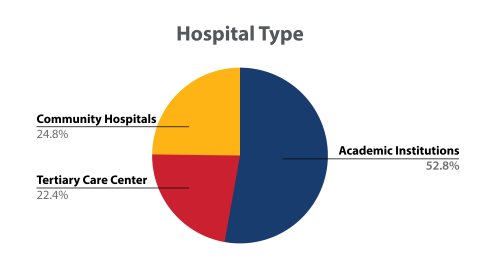
According to the survey responses, a significant majority of the hospitals associated with these heart failure clinics were academic institutions, representing 52.8% of the respondents. In contrast, 22.4% of the hospitals were affiliated with tertiary care centers, while 24.8% were linked to community hospitals.
While initially attributing these demographics to a limited surveyor sample size, further analysis and comparison with Google data confirm the significant lack and subsequent demand for heart failure clinics and services in rural communities. For rural based clinics that participated in the survey, only 28.57% are comprehensive (containing access to most or all the important components of heart failure care) and actively contributing to the field of research. Nearly 71.43% face challenges of comprehensive heart failure care due to insufficient staff and a shortage of heart failure providers.
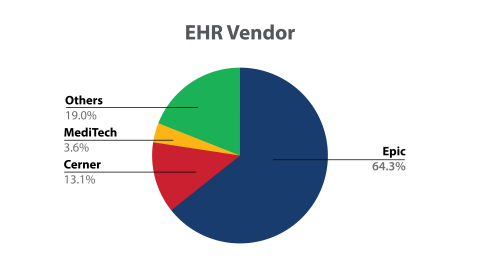
Among the surveyed clinics, there was a variation in the utilization of Electronic Health Record (EHR) software. The most prevalent systems were Epic (used by 64.3%), Cerner (13.1%) and MediTech (3.6%).
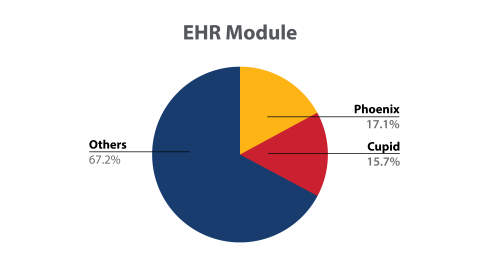
In terms of cardiology modules associated with the EHR vendor, Phoenix was employed by 17.1% of programs and Cupid by 15.7%.
While these clinics varied significantly in the size and scope of practice, the average volume of patients per clinic was 3,368 with an average discharge rate of 1,738 patients per year.
Clinic Staff
The program director was an MD in 87.6% of the clinics and an advanced practice provider or medical provider in 5.6%. Of those surveyed, 4.8% listed a director with a role other than above and 2% of programs listed no clinical director.
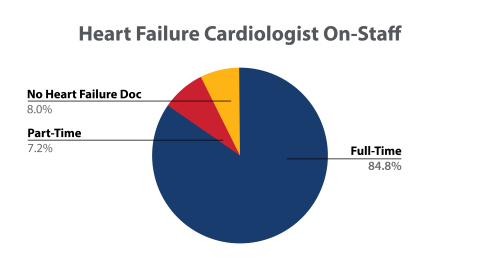
Among the programs surveyed, 84.8% had at least one heart failure cardiologist on staff full-time, 7.2% had a part-time heart failure cardiologist, and 8% of the programs had no heart failure cardiologist employed on staff. Among programs that employed heart failure cardiologists, the average number per program was 5, and 84.8% were board certified.
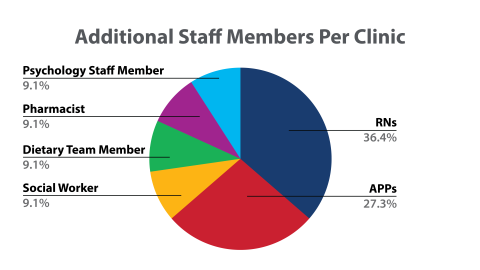
Additional clinical staff included, on average, 4 RNs, 3 APPs, 1 social worker, 1 dietary team member, 1 pharmacist, and 1 psychology staff member per clinic.
Procedures and Services
We examined services considered to be important for a comprehensive heart failure program, including:
- Guideline directed medical therapy (GDMT) titration protocol. An individualized GDMT titration protocol is available on-site at 79.2% of clinics, remotely at 8.8%, and 12% of surveyed clinics do not routinely perform this service.
- Palliative care services. Palliative care services are offered on-site at 69.2%, remotely among 22.8%, and are not provided at 8% of these sites.
- Same day intravenous (IV) diuretic access. Same-day IV diuretic infusions can be done on-site at 72.8% of surveyed clinics.
- Ability to perform standardized functional assessment. Standardized functional status evaluations are routinely performed by 96.39% of survey-responding clinics utilizing New York Heart Association (NYHA) Class. In 64.26%, the 6-minute walk assessment is routinely performed, cardiopulmonary exercise testing (CPET) in 58.63%, and another method (unspecified) is utilized by 6.43%.
- Availability of advanced diagnostic services including coronary angiography, right heart catheterization, and myocardial biopsy. Most sites can perform coronary angiography (94.8%) and endomyocardial biopsy (79.6%).
- Remote patient visits. Remote patient visits are offered at 95.2% of heart failure clinics surveyed, with only 4.8% not providing these services for their patients. However, remote patient monitoring platforms are used at 75.81% of responding heart failure clinics.
- Clinical research. Research is common to many programs and includes provider-initiated protocols (70.8%), multi-center trial participation (76.8%) and other forms of research (4.4%). Ten percent of heart failure clinics do not actively participate in any research. The National Institutes of Health (NIH and RO1) is a funding source for 65% of clinics. Patient-reported outcomes (PROs) are utilized in 51.2% of clinics.
- Access to advanced heart failure therapies including LVAD and transplantation. Single organ transplantation is done at 6.4% of the surveyed clinics and multi-organ transplantation is done at 36% of clinics. Of survey-responding clinics, 74.8% have the capability for LVAD at their centers. For those heart failure clinics that do offer LVAD to their patients as a care option, 52.8% are performing this procedure at an implanting center and 22% at a shared care center.
- Implantable cardiac diagnostics. The routine use of implantable cardiac diagnostics is prevalent in heart failure clinics, with CardioMEMS being employed in 84.74%, OptiVol in 57.83%, and other devices in 2.48%. Seven percent of the surveyed programs currently do not routinely utilize any implantable cardiac diagnostics.
Advanced Heart Failure Care
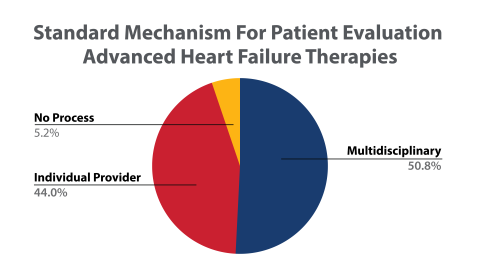
For patients with advanced disease, evaluation for advanced heart failure therapies is done by a formal multidisciplinary team in 50.8% of programs, whereas 44% employ a less standardized approach relying on an individual heart failure provider for evaluation. Approximately 5.2% of surveyed clinics indicated they do not utilize a process to evaluate patients for advanced heart failure therapies.
A limited number of facilities possess the capability to perform and manage patients both pre and post cardiac transplantation. Single organ transplantation is performed at 6.4% of the surveyed clinics, and multi-organ transplantation is available at 36% of the clinics. Access to advanced therapies through a shared care model is available at 22% of these programs and there is no formal access to these therapies at 35.6% of surveyed programs. For patients who may require left ventricular assist device (LVAD) therapy, 74.8% have that capacity; 52.8% being implanting centers and 22% offering a shared care model.
Of the 250 clinics surveyed, 243 provided data regarding the presence of a Specialty Cardiomyopathy Center (SCC). One hundred seventy-five respondents acknowledged the presence of at least one SCC and of those, 62.14% report expertise in the treatment of hypertrophic cardiomyopathy (HCM), 51.03% manage genetic aspects of the disease, 66.67% specifically treat cardiac amyloidosis, and 49.38% report special expertise in the management of cardiac sarcoidosis. In addition, genetic testing is done on sight at 58.4% of surveyed heart failure clinics.
Summary
The HFSA is actively engaged in an ongoing effort to collect and document data from heart failure clinics across the United States. Presently, our database contains approximately 500 distinct organizations and 1,000 unique clinic addresses. HFSA’s goal is to extend this data collection to encompass the additional 2,800 heart failure clinics listed throughout the country. Through this expansion, we aim to gather comprehensive and valuable insights that will aid in enhancing heart failure care and services nationwide.
The data collected in this initial analysis highlights a significant dearth of heart failure services in numerous rural communities. This underscores the critical need for establishing specialized heart failure programs, equipped with specially trained heart failure specialists and clinics, in these underserved rural areas and community-based non-academic centers. By addressing this gap in healthcare access, we can ensure that individuals living in rural regions receive the specialized care they require, leading to improved health outcomes and better overall well-being for these communities.
The data obtained from this survey also identifies lack of uniform participation in research, which may be linked to the limited availability of funding for many of these programs (a higher percentage of community and tertiary clinics indicated having no funding at all for research). Additionally, a significant number of academic institutions reported facing challenges due to insufficient funding for ongoing research endeavors. This financial constraint could potentially hinder the advancement of knowledge and innovation in the field of heart failure care and may necessitate targeted efforts to support research initiatives in all types of heart failure clinics to ensure comprehensive advancements in the management and treatment of heart failure.
This analysis marks a crucial initial step in HFSA’s effort to integrate and standardize heart failure practice throughout our healthcare system. By doing so, we aim to facilitate the exchange of best practices, enhance patients' access to quality care, and promote better adherence to and accessibility of life-saving interventions for the individuals we serve. This concerted effort will pave the way for improved patient outcomes and a more efficient and effective approach to managing heart failure, ultimately contributing to the overall well-being and health of our patient population.
HFSA Heart Failure Clinic Database Task Force
Richard Soucier, MD (Chair), Monica Ahluwalia, MD, Vanessa Blumer, MD, James Dillingham, MMS, PA, PA-C, Katie Ginder, APRN